[This is an OBG (oldie but goodie) post first posted November 4, 2006 - this new post has a few corrections and the fixing of some broken links]
In a
prior post, I highlighted a distinction contemporary mental time-keeping researchers make regarding two general types of human timing systems. Briefly, the
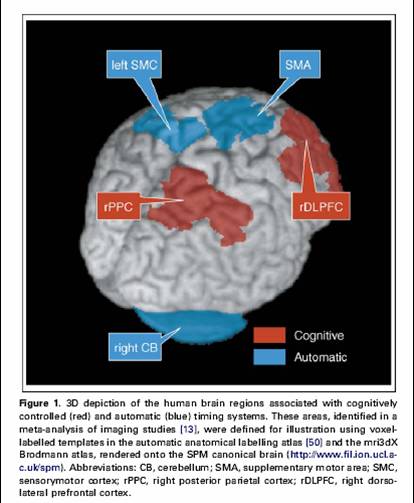
automatic timing system works in the millisecond range of time, is used in discrete-event (discontinuous) timing, and involves the cerebellum. This contrasts with the continuous-event,
cognitively controlled timing system that requires attention and involves the basal ganglia and related cortical structures.
In their article, Lewis and Maill (2006) provide further clarification of how they perceive differences between these two mental timing systems. According to Lewis and Maill,
"it is not any single characteristic, but rather a constellation of several characteristics which determines which timing system is recruited in any particular task." The three task characteristics isolated by these researchers are: (a) the
duration measured, (b) whether or not the timed intervals were defined by
movement and, (c) whether timing was
continuous (e.g. an unbroken series of predictable intervals) or
intermittent (e.g. broken into discrete measurements by the presence of unpredictable irregular intervals).
Lewis and Maill conclude that
"our analysis showed that having any two out of the three characteristics associated with a task type (cognitive or automatic) dramatically increased the probability that the areas associated with that timing system would be recruited. Accordingly, we can think of any task having two or more cognitive attributes (e.g. measuring more than a second, discontinuously, and without relying upon movement) as a ‘cognitively controlled timing task’, and any task with two or more of the opposing characteristics as an ‘automatic timing task’."How does this apply to understanding the brain structures and functions involved in
SMT (synchronized metronome tapping; e.g.,
Interactive Metronome)? [
click here for from info on SMT and IM and my necessary conflict of interest disclosures...just follow the link trails].
Given my understanding (and one personal experience with an SMT intervention), I would hypothesize that SMT interventions most likely tap
both the automatic and controlled cognitive timing systems (and related neurological structures and functions). SMT-based interventions typically involve a motor component (e.g., clapping hands together to the beat), a continuous tone interval, and require responding in terms of milliseconds. These characteristics definitely would be associated with the
automatic timing system.
However, although an individual (during SMT training) is trying to synchronize their tapping in terms of milliseconds, the duration between the continuous tones is more in the range of a second or so. Also, especially during initial stages of SMT, an individual's working memory [see
prior post on the
pacemaker accumulator model of mental time-keeping] is particularly taxed as one monitors the SMT visual and/or auditory feedback provided, makes a decision about whether they are responding "too fast" or "too slow", and then consciously implements a correction to their "beat" behavior. These later characteristics are more characteristic of the cognitively controlled timing system.
So...it is my hypothesis that
both the automatic and cognitively controlled timing systems of mental or interval time-keeping are involved with SMT-based interventions. It is possible that both are significantly active during early stages of SMT training and, with improvement and progress over time, the role of the cognitively controlled system decreases and the automatic system is more responsible. These are only hypothesis and need empirical study.
- Lewis, P. & Miall, C (2006). Remembering the time: a continuous clock. Trends in Cognitive Sciences, 10(9), 401-406.